09.14.14

The Ebola epidemic in Africa has continued to expand since I last wrote about it, and as of a week ago, has accounted for more than 4,200 cases and 2,200 deaths in five countries: Guinea, Liberia, Nigeria, Senegal and Sierra Leone. That is extraordinary: Since the virus was discovered, no Ebola outbreak’s toll has risen above several hundred cases. This now truly is a type of epidemic that the world has never seen before. In light of that, several articles were published recently that are very worth reading.
The most arresting is a piece published last week in the journal Eurosurveillance, which is the peer-reviewed publication of the European Centre for Disease Prevention and Control (the EU’s Stockholm-based version of the US CDC). The piece is an attempt to assess mathematically how the epidemic is growing, by using case reports to determine the “reproductive number.” (Note for non-epidemiology geeks: The basic reproductive number — usually shorted to R0 or “R-nought” — expresses how many cases of disease are likely to be caused by any one infected person. An R0 of less than 1 means an outbreak will die out; an R0 of more than 1 means an outbreak can be expected to increase. If you saw the movie Contagion, this is what Kate Winslet stood up and wrote on a whiteboard early in the film.)
The Eurosurveillance paper, by two researchers from the University of Tokyo and Arizona State University, attempts to derive what the reproductive rate has been in Guinea, Liberia and Sierra Leone. (Note for actual epidemiology geeks: The calculation is for the effective reproductive number, pegged to a point in time, hence actually Rt.) They come up with an R of at least 1, and in some cases 2; that is, at certain points, sick persons have caused disease in two others.
You can see how that could quickly get out of hand, and in fact, that is what the researchers predict. Here is their stop-you-in-your-tracks assessment:
In a worst-case hypothetical scenario, should the outbreak continue with recent trends, the case burden could gain an additional 77,181 to 277,124 cases by the end of 2014.
That is a jaw-dropping number.

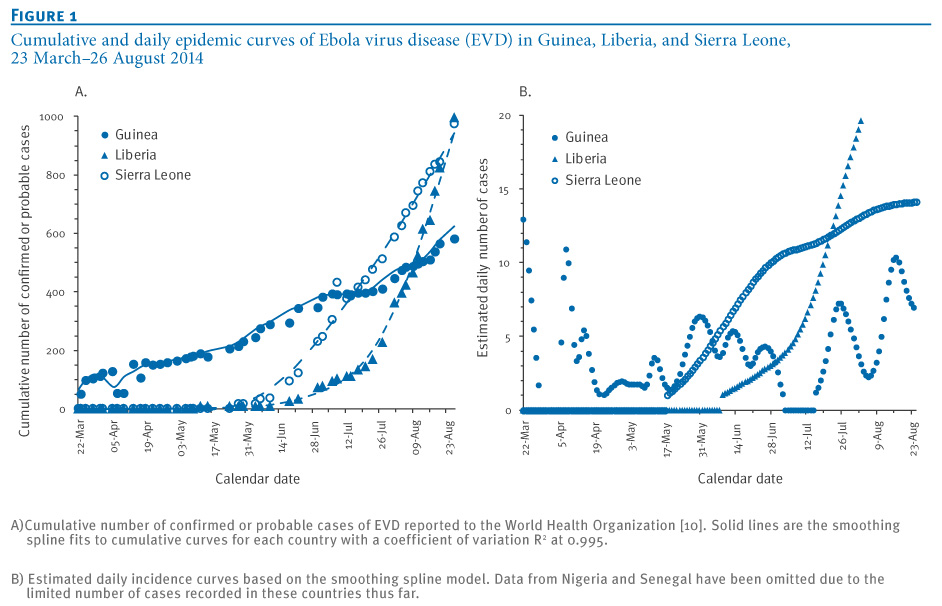
The epidemic curves of the Ebola epidemic; look especially at the line for Liberia. From Nishiura and Chowell; original here.
{kind=link}
What should we do with information like this? At the end of last week, two public health experts published warnings that we need to act urgently in response.
First, Dr. Richard E. Besser: He is now the chief health editor of ABC News, but earlier was acting director of the US CDC, including during the 2009-10 pandemic of H1N1 flu; so, someone who understands what it takes to stand up a public-health response to an epidemic. In his piece in the Washington Post, “The world yawns as Ebola takes hold in West Africa,” he says bluntly: “I don’t think the world is getting the message.”
He goes on:
The level of response to the Ebola outbreak is totally inadequate. At the CDC, we learned that a military-style response during a major health crisis saves lives…
We need to establish large field hospitals staffed by Americans to treat the sick. We need to implement infection-control practices to save the lives of health-care providers. We need to staff burial teams to curb disease transmission at funerals. We need to implement systems to detect new flare-ups that can be quickly extinguished. A few thousand U.S. troops could provide the support that is so desperately needed.
Aid ought to be provided on humanitarian grounds alone, he argues — but if that isn’t adequate rationale, he adds that aid offered now could protect us in the West from the non-medical effects of Ebola’s continuing to spread: “Epidemics destabilize governments, and many governments in West Africa have a very short history of stability. U.S. aid would improve global security.”
Should we really be concerned about the global effect of this Ebola epidemic? In theNew York Times, Dr. Michael T. Osterholm of the University of Minnesota* — an epidemiologist and federal advisor famous for inadvertently predicting the 2001 anthrax attacks — says yes, we should. In “What We’re Afraid to Say About Ebola,” he warns: “The Ebola epidemic in West Africa has the potential to alter history as much as any plague has ever done.”
He goes on:
There are two possible future chapters to this story that should keep us up at night.
The first possibility is that the Ebola virus spreads from West Africa to megacities in other regions of the developing world. This outbreak is very different from the 19 that have occurred in Africa over the past 40 years. It is much easier to control Ebola infections in isolated villages. But there has been a 300 percent increase in Africa’s population over the last four decades, much of it in large city slums…
The second possibility is one that virologists are loath to discuss openly but are definitely considering in private: that an Ebola virus could mutate to become transmissible through the air… viruses like Ebola are notoriously sloppy in replicating, meaning the virus entering one person may be genetically different from the virus entering the next. The current Ebola virus’s hyper-evolution is unprecedented; there has been more human-to-human transmission in the past four months than most likely occurred in the last 500 to 1,000 years. Each new infection represents trillions of throws of the genetic dice.
Like Besser, Osterholm says that the speed, size and organization of the response that is needed demands a governmental investment, but he looks beyond the US government alone:
We need someone to take over the position of “command and control.” The United Nations is the only international organization that can direct the immense amount of medical, public health and humanitarian aid that must come from many different countries and nongovernmental groups to smother this epidemic. Thus far it has played at best a collaborating role, and with everyone in charge, no one is in charge.
A Security Council resolution could give the United Nations total responsibility for controlling the outbreak, while respecting West African nations’ sovereignty as much as possible. The United Nations could, for instance, secure aircraft and landing rights…
The United Nations should provide whatever number of beds are needed; the World Health Organization has recommended 1,500, but we may need thousands more. It should also coordinate the recruitment and training around the world of medical and nursing staff, in particular by bringing in local residents who have survived Ebola, and are no longer at risk of infection. Many countries are pledging medical resources, but donations will not result in an effective treatment system if no single group is responsible for coordinating them.
I’ve spent enough time around public health people, in the US and in the field, to understand that they prefer to express themselves conservatively. So when they indulge in apocalyptic language, it is unusual, and notable.
When one of the most senior disease detectives in the US begins talking about “plague,” knowing how emotive that word can be, and another suggests calling out the military, it is time to start paying attention.
*Disclosure: From 2006 to 2010, I worked part-time at the disease news site,CIDRAP, that Osterholm founded. For that matter, I used to be in a book club with Besser, too.
No comments:
Post a Comment