It just doesn't look like we expected.
This is a story of unconnected dots.
On October 17 2013, a strain of polio endemic to Pakistan first appeared in Deir al-Zor province, Syria. This virus presumably hitched a ride on a ne’er-do-well from Balochistan who thought supporting the Nusra Front would be a good use of his time and likely had no idea he was infected.
On February 12, the U.S. Department of State launched a new Global Heath Security Agenda. The highlight Secretary Kerry’s op-ed on the launch? The 2003 outbreak of SARS, hyped scourge of Asia, with 8,000 known infections and 775 known deaths. The famed Anthrax attacks of 2001, with 17 infections and five deaths, also made an appearance.
On March 11, an infant in Lebanon presented with paralysis. Unlike Jordan, Lebanon has refrained from establishing formal camps for its refugees in an effort to deter permanent residence — a lesson, perhaps, learned from the influx of Palestinians half a century ago.
Priorities
The fact that our “global health security agenda” focuses on future pandemics and deliberate bioterror threats is laughable in the face of reemerging infectious diseases and slaughtered immunization workers. True health insecurity is present globally, and it should not require a mystery test tube and ill intent to be perceived as valid and pressing threat.
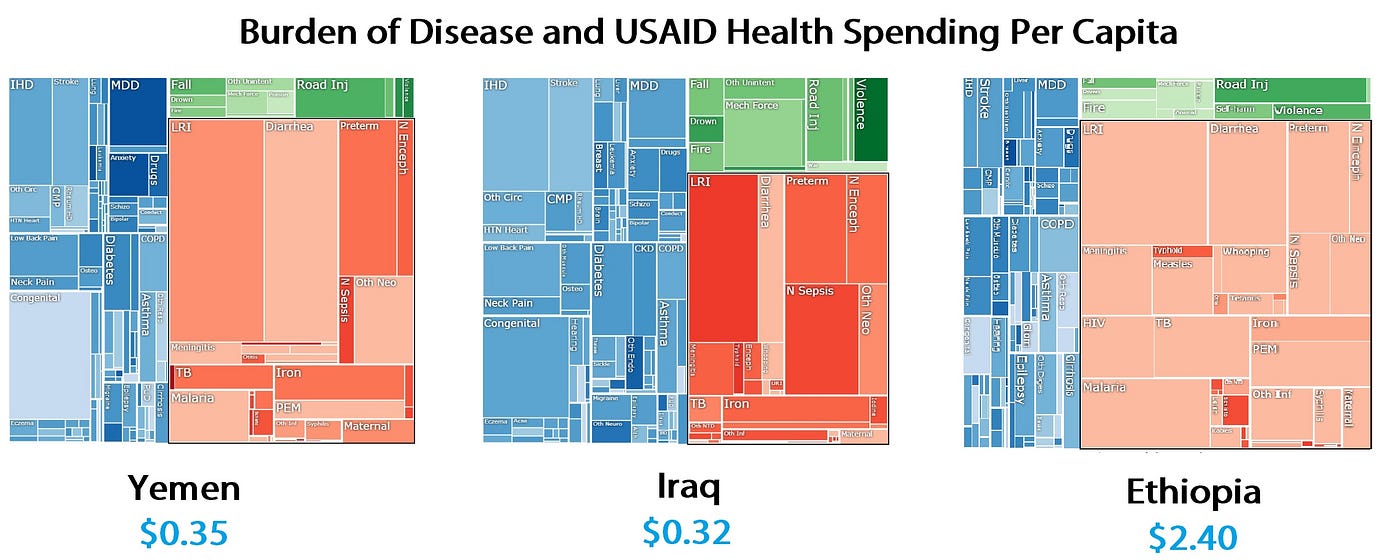
Disease distributions in three countries, with red representing infectious disease. Images from the University of Washington’s Institute for Health Metrics and Evaluation. Data obtained from 2012 State Department budget and CIA Factbook population statistics.
The least health-secure areas are often conflict zones, where the U.S. is heavily invested militarily but where health assistance often lags far behind. There is no better example than the Middle East, where poor health access tends to be masked; statelessness, migrancy, and the sheer law of averages merge oil conglomerates and marginalized masses into a bland middle-income yellow.

View from the Taybeh Health Center in Amman, Jordan, which serves a catchment area of 18,000 Palestinian refugees. Though a model clinic in the region, Taybeh is managed by UNRWA, which is struggling to absorb Palestinian-Syrian double refugees.
27 polio cases have surfaced in Syria since October. That may seem negligible compared to the SARS numbers cited by Kerry, but it represents the tip of an iceberg. When polio “appears,” this often means the case expresses symptoms in the iconic FDR sense — otherwise, it’s rather difficult to tell you have it. The cases easiest to detect, where the virus enters the central nervous system and causes paralysis — obviously signaling a need for prompt medical attention even for people with so much else on their plates — represent roughly 5% of all infections.
27 identified infections imply over 500 total infections. That’s 27 identifiedinfections in a war-torn nation with a decimated capacity for disease surveillance, a barely-existent ability to prevent further spread, and fighters pouring in from an estimated 83 countries. And to top it all off, that same state is hemorrhaging hundreds of refugees by the day.
Lucky thing this is happening on the other side of the world, right?
A health-insecure United States is not a distant threat. It’s here now.
And it will remain as long as health aid is granted to conflict zones as an afterthought to military aid, as long as the idiot proponents of the homegrown anti-vaccine movement are granted airtime, as long as health disparities exist within and between countries, and as long as planes and trains and automobiles propel the modern global economy forward across porous borders.
In short, international health issues will always pose a security risk. Our capacity to prioritize those risks is what will help us remain secure. However, the present agenda does not provide reason for optimism.
Our inability to smother “simple” diseases — those with vaccines and known transmission patterns — is a direct reflection of our global capacity to tame more virulent diseases, many of which we may not anticipate. Diseases do not back down in the face of international condemnation, and they have a pesky habit of ignoring borders.
If the United States crafts a health security agenda around distant pandemics while refusing to take action in places where intervention is politically untenable, we are deluding ourselves. We are all but ignoring the resurgence of a disease from another era in a place where the government actively promotes conditions that facilitate its spread. Meanwhile, we center our panic and policy agendas on milder outbreaks in developed countries. Will we gather the courage to confront health challenges in uncomfortable places when the stakes are higher? The true nature of global health security depends on it, but polio in Syria does not provide an encouraging model.
To continue the conversation, please feel free to engage with me on Twitter@jordanschermer. To learn more about these issues, please check out theSafeguarding Health in Conflict Coalition (with whom I am unaffiliated).
No comments:
Post a Comment